Bridging Women's Career and Health: A Data-Driven View of Filipino Working Women's Well-being
The Challenge
The Philippines has achieved something remarkable: 43% of senior management positions are held by women—the highest rate in ASEAN and among the top globally according to Grant Thornton's 2023 survey. Filipino women lead in retail (72%), education (63%), and food services (62%). They're breaking barriers, climbing corporate ladders, and reshaping what leadership looks like in Southeast Asia.
But beneath these impressive statistics lies a critical question: Are we taking care of the women who are taking care of our economy?
Leadership gains mean nothing if they're unsustainable. And the data reveals troubling patterns: while women advance professionally, their access to preventive health services lags dangerously behind. The result is a fragile progress—women reaching management positions while facing undetected health risks that could derail their careers and lives.
This capstone project asks: How do women's health and empowerment affect their workforce status and career advancement—and what does this mean for sustaining the Philippines' leadership in gender equity?
Our Approach: Linking Health to Economic Participation
Our Batch 11 capstone group built an integrated analytical framework that does something rarely attempted: connecting women's health data with employment data to reveal how health access influences career outcomes. By bringing together datasets that normally exist in isolation, we created a unified view of working women's realities.
The Integrated Data Framework
We analyzed the intersection of health, empowerment, and economic participation through three major national datasets:
Labor Force Survey (LFS) 2023
Employment patterns, working hours, and industry distribution
Occupational categories and managerial representation
806,800 working women respondents
Demographic and Health Survey (DHS) 2022
Preventive health service access (breast cancer, cervical cancer, HIV screening)
Maternal care (prenatal and postnatal visits)
Health insurance coverage and empowerment indicators
ILOSTAT Regional Data
ASEAN-level comparisons for gender parity
Cross-country leadership benchmarks
Regional wage gap analysis
Technical Architecture
Our modern data engineering pipeline unified fragmented government datasets:
Data Collection & Integration
Raw LFS, DHS, and ILOSTAT file ingestion
Multi-format processing (CSV, XLSX, survey data)
Temporal alignment across different data collection periods
Storage & Transformation
ClickHouse cloud data warehouse for centralized analytics
dbt (data build tool) for standardization: region codes, age groups, PSA occupation/industry mappings
Cross-dataset modeling linking health access to employment outcomes
Analytics & Visualization
Tableau dashboards showing health-employment correlations
Regional disparity mapping across health indicators
Industry-level leadership and health access patterns
This reproducible pipeline creates a living analytical system that can be updated as new LFS and DHS data become available, enabling ongoing monitoring of women's health and workforce trends.
Key Findings
Our analysis revealed that Filipino women's remarkable career progress exists alongside troubling health access gaps—creating an unstable foundation for long-term leadership:
1. Women Are Working—But Concentrated in Vulnerable Sectors
The workforce reality:
Women comprise 49.85% of the Philippine workforce
63% of working women are married, balancing careers with family responsibilities
74% are aged 25-54—peak career-building years that overlap with peak caregiving demands
Average age: 42 years old
Industry concentration:
Wholesale & Retail Trade (31%) - often without comprehensive workplace health benefits
Agriculture & Forestry (15%) - informal sector with minimal health infrastructure
Public Administration (8%) - better benefits but bureaucratic access barriers
These sectors, while providing employment, often lack the comprehensive workplace health programs found in corporate environments—meaning the majority of working women have limited employer-supported health access.
2. Leadership Gains Are Real—But Uneven Across Industries
Where women lead:
Wholesale & Retail: 72% of managers are women
Education: 63% female management
Food Services: 62% female leadership
Where women lag:
Transport: 40% - underrepresented in a growing sector
Mining & Quarrying: 33% - barely one-third despite industry expansion
Construction: 32% - male-dominated despite infrastructure boom
The pattern is clear: women dominate management in traditionally "female" sectors (retail, education, hospitality) but remain underrepresented in high-paying technical and industrial fields. This occupational segregation limits earning potential and concentrates women in sectors with weaker health infrastructure.
3. Health Access Is the Biggest Barrier—And Strongly Predicts Leadership
The screening crisis: Family planning remains the most accessed service among working women, but when it comes to preventive screenings:
Women managers are more likely to undergo breast cancer, cervical cancer, and HIV screening than non-managers
National crisis indicators:
65% of breast cancer cases are detected late—when treatment is most difficult and survival lowest
12 Filipino women die daily from cervical cancer—a largely preventable disease
HIV infections among women continue rising, yet screening remains low
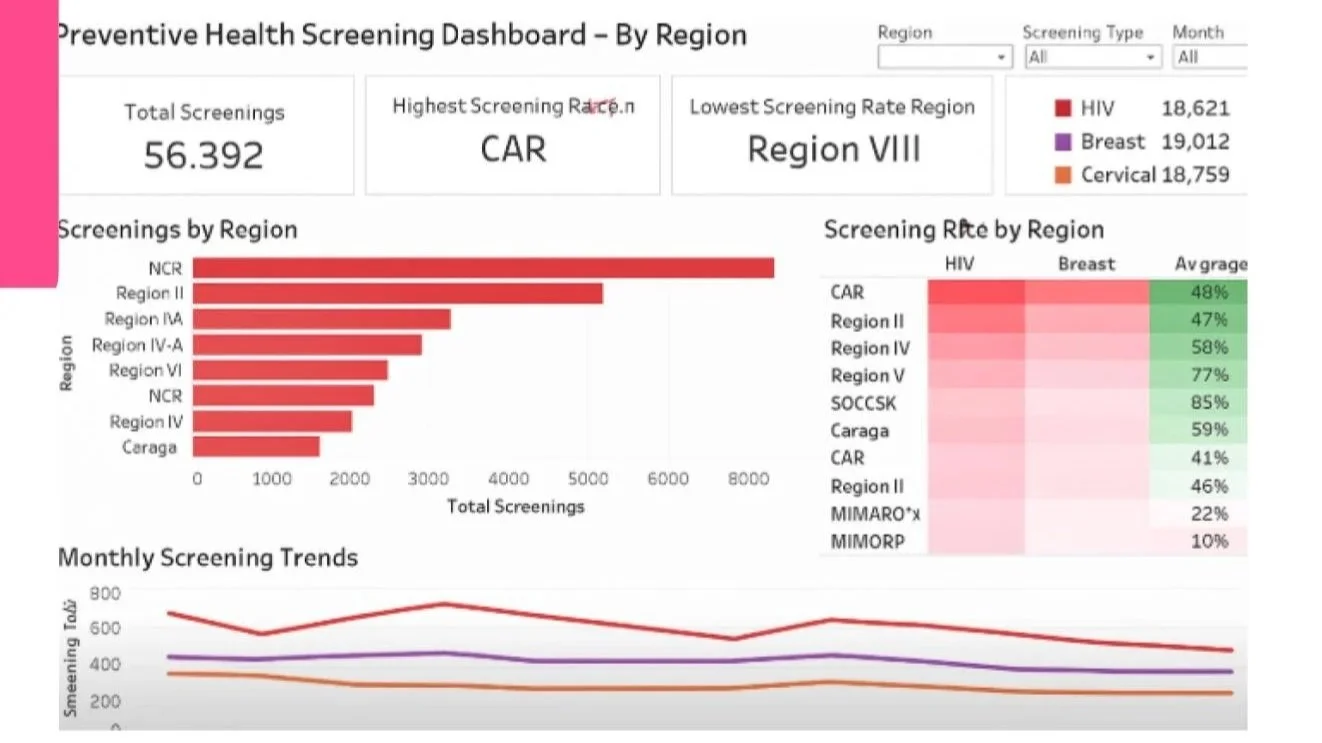
Regional disparities create a two-tier system:
High-access regions (NCR, Caraga, Visayas, Region X, CAR):
38-40% uptake across preventive screenings
These regions can serve as benchmarks for raising women's preventive care nationwide
Low-access regions (Eastern Visayas, Davao Region, MIMAROPA, SOCCSKSARGEN):
Below 25% screening uptake
Women managers are "left behind" with the widest health gaps
Represents the biggest opportunity for impact
The correlation: Regions with stronger preventive health access tend to show higher female managerial representation. This isn't coincidental—women with better health access are more likely to stay employed, advance, and lead.
4. The Dual Burden: Career Peak Meets Caregiving Peak
63% of working women are married, and 74% fall in the 25-54 age bracket—the years when career advancement opportunities peak but also when caregiving responsibilities intensify:
Young children requiring attention
Aging parents needing care
Household management falling disproportionately on women
This dual burden affects:
Screening uptake: Working women delay health checkups due to time constraints
Career continuity: Health issues discovered late force career interruptions
Long-term advancement: Untreated health conditions limit sustained leadership capacity
The data suggests that without adequate health support systems, the very years when women should be advancing most rapidly become years when they're most vulnerable to dropping out or plateauing.
5. The Fragility of Progress
The Philippines leads ASEAN in women's management representation—but this leadership is fragile without equitable health access. Consider:
A woman reaches management in her 30s-40s
She delays preventive screenings due to work and family demands
A health condition goes undetected until it's advanced
Treatment requires extended leave or career exit
Her leadership position is lost, not due to lack of competence, but due to preventable health crisis
This pattern repeats across regions with low health access, undermining decades of gender equity progress. Leadership representation can't be sustained if the women achieving it can't access the healthcare needed to stay healthy and working.
Impact & Recommendations
This integrated health-employment analysis provides actionable intelligence for government agencies, corporate HR departments, women's advocacy organizations, and regional health planners. Our framework enables evidence-based strategies to sustain women's workforce gains.
Core Recommendation Framework
Address the systemic barriers preventing working women from accessing preventive health services—particularly in regions and sectors showing the widest gaps. Rather than treating health and employment as separate policy domains, recognize that sustained workforce participation depends on accessible, appropriate healthcare.
The following recommendations identify what systemic issues must be tackled, not prescriptive solutions—recognizing that effective interventions require stakeholder consultation and context-specific design.
1. Prioritize Health Access in Low-Uptake Regions
The Challenge: Eastern Visayas, MIMAROPA, Davao Region, and SOCCSKSARGEN show screening uptake below 25%—leaving women managers and workers at heightened risk.
What Must Be Addressed:
Geographic accessibility barriers: Why women in these regions cannot physically reach screening facilities
Service availability gaps: Whether adequate screening infrastructure and trained personnel exist
Awareness and cultural factors: What prevents women who could access services from doing so
Economic barriers: Whether out-of-pocket costs deter even employed women from seeking care
Interventions must tackle why these regions consistently underperform despite having working women populations comparable to high-access areas.
2. Replicate Success from High-Performing Regions
The Opportunity: NCR, Caraga, Central Visayas, Region X, and CAR achieve 38-40% screening uptake—demonstrating that better outcomes are possible.
What Must Be Understood:
Infrastructure factors: What screening facilities, outreach programs, and service delivery models exist in these regions
Policy enablers: Whether local government health budgets, public-private partnerships, or employer programs contribute to success
Cultural acceptance: How health-seeking behavior is encouraged and normalized in these contexts
Rather than inventing new approaches, scaling what already works in high-performing regions could accelerate progress in lagging areas—but only after understanding what makes those models successful.
3. Address Workplace Barriers to Health Access
The Challenge: 63% of working women are married, 74% are aged 25-54, and most work in sectors without comprehensive health benefits—creating time, financial, and logistical barriers to preventive care.
What Must Be Addressed:
Time constraints: How work schedules prevent women from attending screenings during clinic hours
Employer support gaps: Why most Philippine workplaces lack health programs beyond PhilHealth
Sector disparities: How women in retail, agriculture, and informal sectors have fundamentally different health access than those in corporate environments
The dual burden reality: Why women managing both careers and caregiving responsibilities deprioritize their own health
Interventions should address why employment—which provides income and theoretically better access to services—paradoxically creates barriers to actually using preventive care.
4. Build National Women's Health & Workforce Monitoring Systems
The Challenge: Health and employment data exist separately, making it impossible for policymakers to see how health access affects workforce participation and leadership advancement.
What Must Be Developed:
Integrated reporting frameworks: Systems that link health service utilization with employment outcomes
Regional tracking mechanisms: Monitoring that identifies emerging health access gaps before they widen
Evidence-based resource allocation: Data infrastructure enabling targeted health investments in regions and sectors with the greatest need
The goal isn't more data collection—it's creating systems that connect existing data to inform strategic decisions about where health investments will most strengthen workforce participation.
5. Integrate Women's Health into Workforce Development Strategy
The Challenge: Government and corporate workforce development programs focus on skills training, leadership development, and career advancement—treating health as a separate domain rather than a foundational requirement for sustained participation.
What Must Change:
Policy integration: Why workforce development agencies don't coordinate with health service providers
Corporate retention strategies: How companies can recognize that preventive health support is retention investment, not just benefit expense
Long-term planning: Whether national economic development plans account for the relationship between women's health access and labor productivity
Effective strategies must acknowledge that you cannot build a sustainable female leadership pipeline while allowing preventable health crises to derail women's careers.
Why This Matters
The Philippines has achieved something remarkable: 43% of senior management positions held by women, ranking first among 28 countries globally. This didn't happen by accident—it's the result of progressive policies, cultural factors supporting female leadership, and decades of investment in women's education.
But this achievement is fragile. Every year, working women delay cancer screenings because they can't take time off work. Every month, women in low-access regions face preventable health crises that could have been caught early. Every day, talented female managers risk losing careers they worked years to build—not because they lack competence, but because they lack accessible healthcare.
The data shows a clear pattern: Women with better health access are more likely to stay employed, advance, and lead. This means that sustaining the Philippines' leadership in gender equity isn't just about hiring and promoting more women—it's about ensuring the women who reach leadership positions can stay healthy enough to sustain those roles.
The Path Forward
This capstone demonstrates that the technical capability exists to link women's health and employment data, revealing patterns that inform strategic interventions. Our Batch 11 group built a working analytical framework using publicly available datasets and modern data tools.
The question isn't whether we can identify where and how health access affects women's careers—we can, and this project proves it. The question is whether policymakers, employers, and health system leaders will use this intelligence to protect the hard-won gains in women's leadership.